Understanding your baby’s diagnosis
Medically reviewed and edited by Marisa Schwab, MD | Written by Emily Lake, PhD |
Last updated 03/23/2026
This page has information about the most common presentations of congenital lung malformations.
Congenital means a condition that is present at birth and a lung malformation means that part of the lungs did not develop properly.
My diagnosis is…
-
CPAM (previously called CCAM) is an abnormal mass of lung tissue, normally affecting one lung lobe. The CPAM can be macrocystic, meaning it is made up of one or more large cysts, solid, or microcystic, meaning it is made up of many smaller cysts. The CPAM is part of the lungs and connected to the lung’s blood supply.
CPAM is the most common type of congenital lung malformation.
-
BPS is the second most common congenital lung malformation after CPAM. Like CPAM, a BPS is an abnormal growth of lung tissue, but unlike CPAM, the mass is not connected to the lung’s blood supply.
A sequestration means something that is separate. In the case of BPS, it is the blood supply that is separate from the pulmonary (lung) system, and there is no communication with the airway. The BPS is connected instead to a nearby systemic vessel, normally the aorta.
A BPS can be intralobar (meaning the mass is within or part of a lung lobe, but with a separate blood supply) or extralobar (meaning the mass is not part of the lung structure at all).
-
Congenital lobar emphysema, also known as congenital lobar overinflation, is a rare congenital lung malformation (CLM) where part of one lung becomes overinflated because air can get in—but not out—of that area.
This happens very early in development, probably before the 10th week of gestation, when the cartilage or structure of the bronchus (the main airway branch) doesn’t form normally. The airway can be too narrow, soft, or “floppy,” which acts like a one-way valve. Air enters the lobe during inhalation but becomes trapped during exhalation. As a result, that lobe expands too much and can press on the other lobes or nearby organs.
CLE most often affects a single lobe of the lung, most commonly the left upper lobe, but it can occur in any lobe.
-
CBA is a rare congenital lung malformation where a segment of the airway (bronchus) didn’t grow normally.
This happens very early during pregnancy, sometime before the 10th week of gestation. The result is that a small area of lung cannot communicate properly with the rest of the airways. Because air can’t move in and out normally, that area of lung may become over-inflated.
CBA can affect one small segment or an entire lung lobe. It most commonly affects the upper lobes, but it can occur in any part of the lung.
-
A mass can show characteristics of both CPAM and something else, normally BPS, but sometimes CLE or CBA. These are called hybrid lesions. The only way to know the exact characteristics of the lung mass is when a pathologist looks at it after surgery. Hybrid lesions are treated the same as other lung malformations.


A CPAM lesion affecting the lower left lobe
An intralobar BPS lesion affecting the lower left lobe
Is this cancer?
No. Congenital lung malformations are not cancers.
For CPAM and BPS, the masses are benign: they are not cancerous. There is thought to be a very small risk of cancer, but research is needed to determine whether it’s because the malformations may become cancer in the future if not removed, or whether a childhood lung cancer (called pleuropulmonary blastoma or PPB) is misdiagnosed as CPAM or BPS.
There is no known pathway for CBA or CLE to develop into cancer. There may be an increased risk of cancer with CPAM, and some patients have hybrid lesions, meaning both CBA with CPAM or CLE with CPAM. More research is needed to truly understand the relationship between CPAM and cancer.
How do you know what type of lung malformation it is?
The radiologists and surgeons will be able to give you a good guess based on prenatal imaging. The CT (normally a few months after birth) will give the clearest picture. However, the only way to know for sure is for the mass to be studied by a pathologist after it is removed during surgery. A number of these malformations may be a mix of two types of lesions. All of these lesions (CPAM, BPS, CBA, CLE) are treated the same way.
Can a mass be both CPAM and something else?
Yes. A mass can show characteristics of both CPAM and another kind of lung malformation (normally CPAM and BPS). These are called hybrid lesions. Again, the only way to know the exact characteristics of the lung mass is when a pathologist looks at it after surgery.
Is CCAM something different?
No. CCAM is just the old term for CPAM.
How are lung malformations diagnosed?
Nowadays most congenital lung malformations are diagnosed during pregnancy at a routine 20 week ultrasound scan. The area of malformation appears much brighter than healthy lung tissue on an ultrasound up until around 28 weeks. Imaging technology is getting better and better at detecting lung abnormalities more accurately and earlier than ever before. Previously, CPAM or BPS would never be detected (especially if the mass caused no problems) or only be discovered incidentally, normally following an X-ray or other imaging study after repeated chest infections.
How common are lung malformations?
Nobody knows exactly, but being diagnosed with a congenital lung malformation is still uncommon, even with technological advances leading to much better detection rates. Congenital lung malformations altogether are thought to impact 1 in 2,500 live births.
What is the prognosis for someone born with a congenital lung malformation?
The prognosis is excellent. In the overwhelming majority of cases a lung malformation will not affect a child’s life expectancy or quality of life. In some rarer cases, the lung malformation presents more serious complications during the pregnancy or immediately after birth. In particular, if the lung mass grows very quickly, or is very large, fluid can build up in nearby organs. This build up of fluid is a rare but very serious condition called hydrops. When the lung malformation is more dangerous, the pregnancy must be extremely carefully monitored by specialists.
Will the baby be able to breathe at birth?
In 90% of lower risk cases, babies with a congenital lung malformation are asymptomatic at birth, meaning they breathe normally without needing oxygen, and act like other babies. In other cases a baby may be symptomatic, meaning they need some help or breathing support early on. In rare cases surgery may be needed soon after birth.
What is the treatment for lung malformations?
Treatment differs by where in the world the patient is receiving medical care.
In the US, most cases are nowadays spotted during pregnancy. In these situations, the standard practice is to monitor the size of the lung malformation during the pregnancy to make sure it is not affecting the baby's other organs. The baby will then have surgery to remove the CPAM or BPS when they are at least a few months old, although in some rarer cases surgery has to happen sooner.
In other parts of the world (like Europe and Australia) the lung malformation will still be monitored closely during pregnancy, but doctors follow more of a “wait and see” approach and don’t always recommend surgery for every patient.
What causes lung malformations?
Nobody knows for sure but they are not caused by anything the mother did, or didn’t do, during pregnancy.
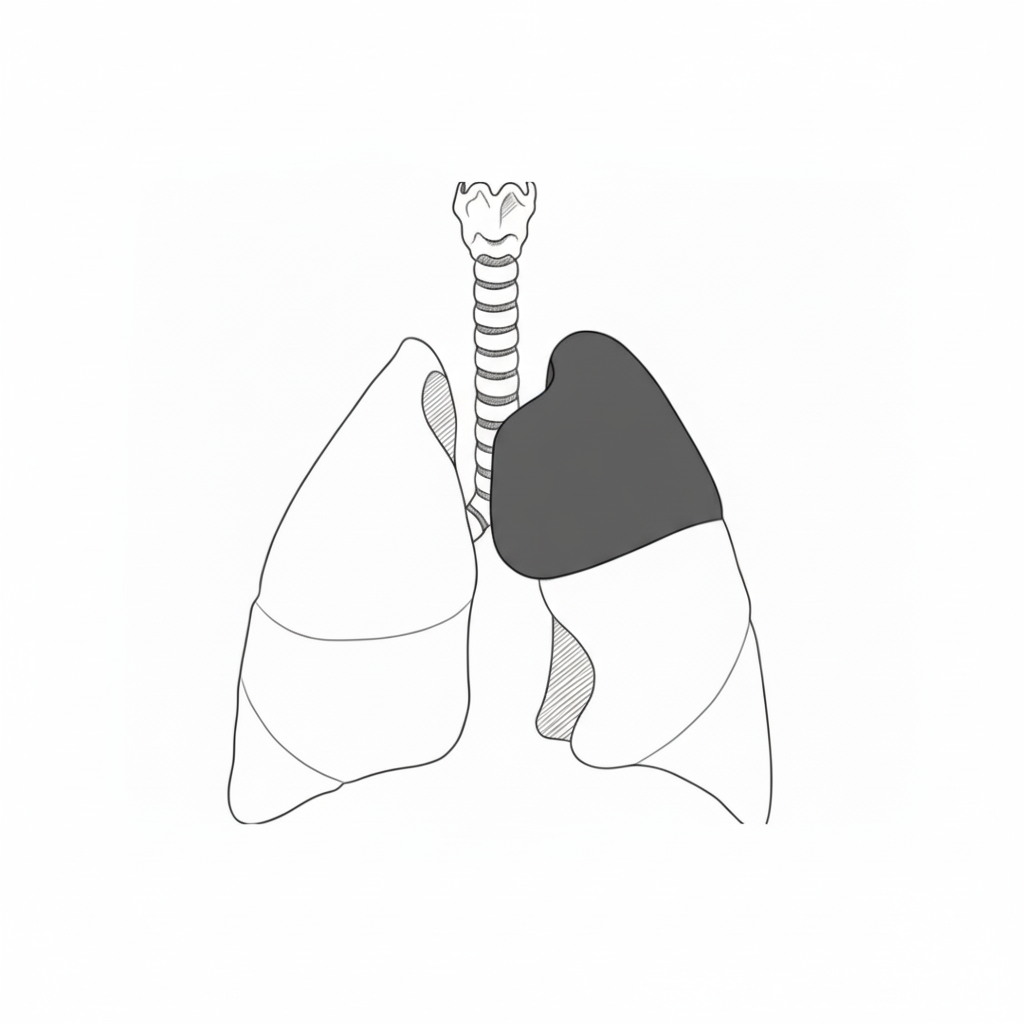
Congenital lobar emphysema affecting the upper left lobe

A CPAM as it appears on a prenatal ultrasound. The lesion is brighter than the surrounding healthy lung tissue.
Jordan (2016) Sonographic Appearance of Congenital Pulmonary Airway Malformations
Recommended reading
Our parent guides by CLM type
What do we really know about lung malformations?